
Common Hip Damage: Repair and Replacement
@Barun Kumar Basak, 1971 Mechanical Engineering
Preface
This composition is the third in the series of very common health related public interest matters, after (1) Phaco-Emulsification (cataract) Eye Procedure and (2) Nasal Septoplasty, by the same author. These were procedures undergone by the author himself and related studies were made before, during and after the events, to understand them better. A mechanical engineering graduate by (only) basic qualification, the author is convinced about all medical invasive procedures in body being essentially structural corrections, modifications, adoptions, and supporting by means of specially engineered materials, tools, machines, components and technology. The author is of the firm view that the knowledge earned from his direct exposure to such procedures and corresponding studies made, may better be shared with common people who are either existing or future possible patients or their family members, or friends, so that there is a clearer view of the prescribed actions by the doctor.
Background
A very active super senior family member of the author had tripped inside her home and damaged hip. She underwent surgery at a steel plant hospital and was rehabilitated to start walking with a stick. After sometime she experienced pains in internal organs, which was investigated to be parts of the implants getting loosened and piercing organs. Doctors found the reason to be intense osteoporosis crumbling all bone mass, unable to hold the implanted screws in position. Further surgery removed all the screws and plates to give her relief from possible punctures, while she lived the most cruel bed-ridden life thereafter. The author wondered whether she tripped to break the bone or whether crushed bones made her fall.
Thereafter, there have been an accidental fall to the spouse needing total hip replacement and two very close friends with hip fractures requiring repairs with plate, rod and screws. Origin of the plan for this article are these events and the related studies made by the author.
Femur In Bine Anatomy
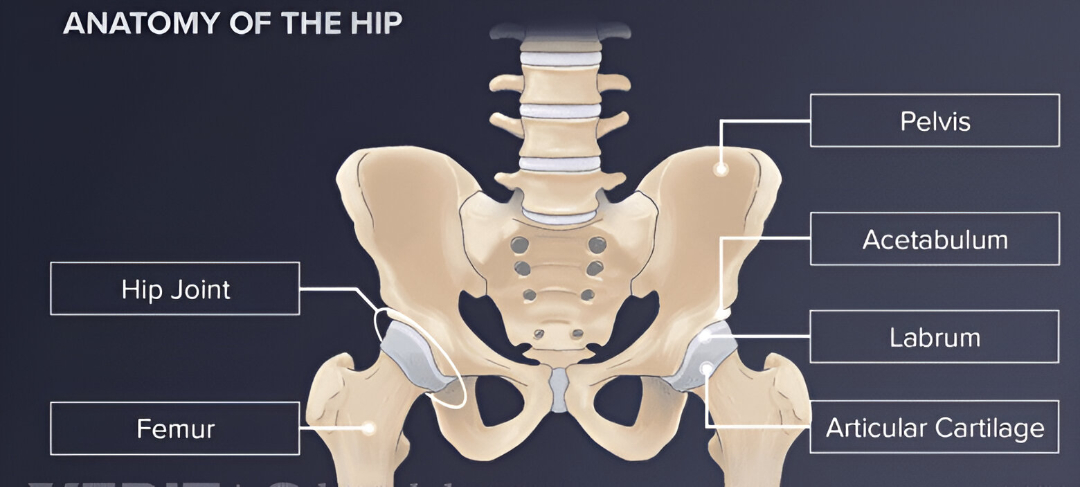
“Femur” or Thigh Bone is the only bone in the upper leg, joining the hip with the knee. In humans, femur is the largest and thickest bone.
It is typically around 450 mm (18-inches) long in a fully grown adult, connecting pelvic bone at hip joint with lower bones at knee joint. By shape it is like a shaft in the middle with two rounded ends. Top of the femur fits into a socket or “acetabulum” in the pelvis at “hip-joint”.

Femur plays a key role in standing and in moving while supporting muscles, ligaments and parts of circulatory system. It is surrounded by thigh muscles including quadriceps and hamstring. Bottom of the femur connects with shinbone or “tibia” and the kneecap to form the knee. The two femurs converge medially towards the knees, where they articulate with the proximal ends of shin-bone.
“Head” of the femur is shaped like two-third of a sphere (ball) which articulates within the acetabulum or the socket in a pelvis notch. Head of the femur is connected to the shaft by a 40-50 mm neck or “collum” set at an angle of about 130-deg.
Femur Damages – Main Types
Femur – the longest, heaviest and strongest bone in the body, naturally takes the strongest force to break it. They happen in accidents of cars or motorcycles. A broken femur is a serious injury demanding immediate medical intervention to realign the bones of the leg and to preserve damaged muscles, tendons, ligaments. Once broken, damaged femur may take months to heal.
Three main types of damages are :
1) Proximal Femur fractures involving upper portion of the bone near Hip Joint
2) Femoral Shaft fractures involving middle part of the bone, with severe injuries
3) Femur fractures involving just above the knee
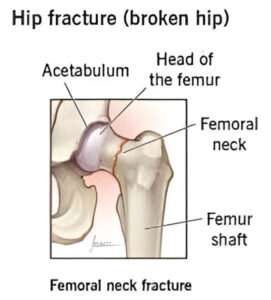
Hip Fracture – Proximal Femur
A “Hip Fracture” is a break that occurs in the upper part of the femur, at the femoral neck or (rarely) the femoral head. Symptoms include pain around the hip, particularly with movement, shortening of the leg. Usually, the person cannot walk. A hip fracture is basically a femoral “neck” fracture and Trochanteric fracture. Such fractures most often occur as a result of a fall. Femoral “head” fractures are a rare kind of hip fracture that may also be the result of a fall, but are more commonly caused by severely violent incidents such as in traffic accidents.
Risk factors may include osteoporosis, or due to tobacco smoking or alcoholism or taking many medications and sometimes also cancer. These are pathological effects.
Women folk are more affected than men. About 15% of women break their hip at some point in life. Hip fractures become more common with age.
Diagnosis is by X-Ray. CT-Scan or MRI is sometimes required when X-ray fails to diagnose a fracture in spite of strong clinical suspicion. Bone Density checks are required later to treat underlying osteoporosis. Most Hip Fractures are treated surgically. Surgery is generally recommended as early as possible.
One of the options for surgery may be Hip Replacement (Hip Arthroplasty) which may be total or partial hip replacement for older adults. THR (Total Hip Replacement) is adopted for elderly patients who are independently mobile, medically fit and still active. Hemiarthroplasty or Partial Replacement by implants when full hip joint is not required to be replaced.
Other (younger) patients may be advised for fixation in situ of the damaged bone with a metal implants like plates, rod, screws or pins in ORIF (Open reduction and internal fixation) procedure to secure the fractured bone pieces. Some people live with these fasteners inside forever, while some others can get them removed after full healing.
For low-grade fractures, standard treatment is fixation of the fracture in situ with screws or a sliding screw/plate or screwed blade/rod device. This procedure is also applicable for displaced fractures after the fracture has been reduced. This process of implanting is referred as “Cannulated Screw Fixation”. However, when the fracture cannot be reduced, “Dynamic Hip Screw” implanting is adopted which permits controlled dynamic sliding of the femoral head. This process is common for older osteoporosis patients. This DHS process allows for both primary healing of the femur and also cells joining at boundaries thereby making a robust joint.
Trochanteric fractures are treated by internal fixation of the fracture with Dynamic Hip Screw (DHS) or Proximal Femur Nail (PFN).
Arthroplasty – Total Hip Replacement (THR)

THR – Arthroplasty involves replacing both the socket in the hip and the thigh side of the joint with an artificial joint implant. Hemiarthroplasty (partial hip replacement) leaves the socket intact, replacing only the thigh side.
In THR, the damaged bone and cartilage are removed and replaced with synthetic components called implants.
• The damaged femoral head is removed and replaced with a metal stem that is placed into the hollow central cavity of the femur bone. The femoral stem may be either cemented or “press fit” into the bone.
• A metal or ceramic ball is placed on the upper part of the stem. This ball replaces the damaged femoral head ball that was removed.
• The cartilage surface of the socket (acetabulum) is removed and replaced with a metal socket. Screws or cement are sometimes used to hold the socket in place.
• A plastic, ceramic, or metal spacer, also called a “liner”, is inserted between the new ball and the socket to allow for a smooth gliding surface.
Hemiarthroplasty – Partial Hip Replacement
Partial Hip Replacement or Hemiarthroplasty involves replacing the femoral head with a prosthesis whilst retaining the natural acetabulum and acetabular cartilage. Total hip replacement involves the replacement of the acetabulum in addition to the femoral head.
Femoral Shaft Fracture
Fractures of the femoral shaft are quite common injury, often associated with great trauma and can be life-threatening. They often result from high-energy mechanisms such as motor vehicle collisions with threat of possible limb shortening and deformities if not treated correctly.
Femoral Shaft Damage Treatment and Repair
Most femoral shaft fractures require surgery to heal. Very young children are sometimes treated with a cast.
Surgical fixation with intramedullary nailing is possibly considered better. Other surgical techniques include plate open reduction internal fixation (ORIF) techniques and external fixation (EF).

Intramedullary Nailing
During this procedure, a specially designed metal rod is inserted into the canal of the femur. The rod passes across the fracture to keep it in position.
External Fixation (EF)
Metal pins or screws are placed into the bone above and below the fracture site, with the pins and screws being attached to a bar outside the skin. This device is a stabilising frame that holds the femur in position. An EF is a temporary solution until the patient is healthy enough for the final surgery. Sometimes an EF is left on until the femur is fully healed
Distal Femur Fracture
Fractures of the thigh bone that occur just above the knee joint are called “Distal Femur Fractures”. The distal femur is where the thighbone flares out like an upside-down funnel. The distal femur is the area of the leg just above the knee joint.
Distal Femur Corrections
Most of the time, surgery is needed to treat distal femur fractures. Sometimes, doctors use an “external fixator” (pins and bars outside the skin) to line up the bones and help with pain and movement until the swelling goes down enough for surgery. The surgery involves in making cuts on the front, outside, or inside of the knee and thigh. The bones are put back in place with use of metal plates, screws, or a rod to hold them securely.
Damage Prevention
Risk Factors at Home
Many falls are the result of hazards like slippery or wet surfaces, poor lighting, inadequate footwear, lack of handrails, and cluttered pathways in the home.
Most fractures are the result of a fall in the home, usually related to everyday activities such as walking on stairs, going to the bathroom, or working in the kitchen.
Creation of safe conditions is most important to prevent accidental fall
Well-lit rooms, clear passage, handrails, ergonomic designs, anti-slip floors
Lifestyle Changes
Maintaining health and staying physically active may help reduce risk of falling,
and also monitoring the following factors among others –
Annual eye examination to correct vision
Addressing cardiac and blood pressure problems
adequate dietary Calcium and Vitamin D
Discard smoking and restrict alcohol intake
Check side effects of medications, since both fatigue and confusion increase risk of falling.
Checking and control of weight
Exercise program for agility, strength, balance, coordination
Immediate Management
It needs great deal of caution and care to attend to a femur damaged person. No movement of the injured area, unless it is a must. Following may be considered as immediate help :
Stop any bleeding.
Apply pressure to the wound with a sterile bandage or a clean piece of cloth
No attempt to try to realign the bone or push a bone that’s sticking out back in.
Apply ice packs to limit swelling and help relieve pain; wrap the ice in a cloth
Treat for shock; lay the person down with head slightly lower than the trunk, raised legs
Rehabilitation
A gentle rehabilitation program commences after surgery to help strengthen the muscles around post-operative hip and to regain the range of motion. Usually within the next 24 hours, the physio- therapist helps start walking a few steps at a time, with a walker. With healing of wounds, patient progresses from walker to crutches or to a stick. As medications continue for a while, muscle exercises as directed by physio-therapist, become a routine. Ice packs may be used in case of pain. Walking, remaining active and practicing the required exercise are the quickest ways to full recovery. No attempt during this period to put the femur to test.
Generally it requires 3 to 4 months to come to normal life. Initially load carrying, kneeling or squatting are totally forbidden as also consuming alcohol, soda, salt, caffeine, sweetened beverages and completely stopping smoking too. A well-balanced diet needs to be maintained with egg, chicken, green vegetables, fruits.
Rehabilitation also includes investigating underlying deficiencies, illness, osteoporosis, cancer, and other factors causing the fracture for their corrective or restrictive measures. It is to be always kept in mind that no implant can offer a full life as compared to original body organs which have automatic rejuvenation capability. Implants are, in any case, made of metals, ceramics or plastics or other synthetics with their own limitations, wears and tears and sustained one-way deteriorations. They need extreme care in use in post-operative life.
Conclusion
A general outline has been attempted in this composition for some kind of understanding surely needed by general people with interest like me or anyone around. This is not claimed to be any original paper, like most books also are. This can rather be defined as a synthesis of personal experience, studies and analysis made and also collected from sources. Author would be happy if it can create interest and satisfaction among readers and for raising queries.
References and Acknowledgements
Wikipedia, Cleveland Clinic, Mayo Clinic, Stryker Corp, DePuy Synthes, Miraclus Orthotech, and many others.
Inspirations
Inspirations have been greatly derived from sufferers and champions – Late Kamalini Bhor, Mother In-law; Sm. Shipra Basak, life partner; Er. Pradip Kr Mukherjee, college friend; Er. Bhudeb Das, school friend. They liberally permitted sharing their medical data and documents.
Grateful Tribute
The author is immensely grateful to Dr. Saumitra Misra, M.S.(Ortho), FRCS, renowned contemporary Orthopaedic Surgeon who cared for Shipra Basak for her THR Arthroplasty in August 2012 and for Pradip Kr Mukherjee for Helical Blade Nailing (ORIF) in September 2024. Former is undergoing sustained treatment for bone density and consolidation under him, while latter has completed rehabilitation post surgery.













Thanks to the author(Er. Basak ) for his well researched composition on this subject on orthopedics in a very lucid manner. An interesting read and surely a good guide for layman like us.